Aberrations
of the Equine Estrous cycle
 166-171 166-171

True polyestrous
Note the year around cycles in this mare.
- Theoretically all mares at equator will have
equal light and dark year around, so they should not have an
anestrous period.
- In reality, about 20 % of mares in the Northern
Hemisphere will cycle the year round. Whether this is an
insensitivity to melatonin is unknown.
Silent heat
- This is when the mare fails to show behavioral
signs of estrus, even though normal physiological estrus is
occurring.
- Examination of these mares shows the
progesterone to be low at estrus and rise with a normal ovulation.
- The incidence of this syndrome seems to vary
with the efficiency of the teasing program, but can be up to 15%
even on a well managed farm.
- Mares that are prone to have this problem are
shy mares, maiden mares, and foaling mares (caused by
over-protectiveness of the foal).
- Poor heat detection is usually to blame,
however.
- Diagnosis
- Determine by rectal palpation and/or ultrasound
that the mare is cycling normally.
- Evaluate the teasing program to ensure that
teasing is optimized.
- Progesterone assays may also help in
determining if the mare is truly ovulating and forming a corpus
luteum.
-
Treatment
- Careful teasing may increase the chance of
catching the mare in heat.
- You may want to suggest varying the heat
detection methods. Use individual instead of group teasing, change
stallions to see if the mare will react to a different stallion.
- Daily palpation or you may need to palpate
every 12 hours because of the confusion between follicles and corpus
hemorrhagicum.
- Daily or every other day ultrasound exams.
Ultrasound exams are a good method to tell when a mare is in estrus
because of the characteristic appearance of the uterus of a mare in
heat.
- You can use prostaglandin to bring the mares
into an estrus that is more predictable to time (i.e. they will watch
for it more closely)
- Artificial Insemination (AI) or appropriate restraint for natural cover
may be required. Most of these mares will break down for breeding
when they are twitched. You really hold your breath though when you
walk the stallion up to a kicking mare that you say is in heat based
on your palpation.
Multiple ovulations
- Up to 24-26% of ovulations are multiple.
(Somewhat breed dependent, some breeds, e.g. Warmbloods may have 35%
double ovulation rate). 99% are double and only 1% have more than 2
ovulations.
- There is a 73% incidence within individual
mares.
- Generally there is about 1 day between
ovulations. Progesterone rises after the second ovulation.
- The problem with multiple ovulations is that
they lead to twin pregnancy, which result in a high percentage of
abortions due to placental insufficiency.
- Diagnosis is based on palpation and/or
ultrasound of two follicles at estrus forming two corpora lutea.
Note the multiple ovulations as noted by the arrows in May and June.
-
Treatment
- You can short cycle all mares with twin
ovulations with prostaglandin to bring them back into estrus, which is the way some farms handle
the condition.
- You can breed to the second ovulation, because
the oocyte only has a 12- 24 hour life span so only the second
oocyte should fertilize. Problems with this approach include reduced
estrous behavior of the mare and decreased uterine defense
mechanisms because the CL from first ovulation is producing
progesterone.
- You can take your chances and worry about twins
later when you do an early pregnancy check for twins. This is
probably the most common approach now. At < 16 days you can crush
one of the twins.
Diestrous ovulations
- Ovulation can occur in the luteal phase (high
progesterone) with no signs of heat.
- A 24 % incidence reported, and these mares have
been bred and become pregnant from the diestrus ovulation.
- You must rule out silent heat by palpation of
the cervix and uterus and ultrasonography, or using progesterone
analysis.
Note the diestrous ovulations indicated by the
arrow during high progesterone in July.
Effect
- If the ovulation is early in the cycle there is
no effect on next cycle because the corpus luteum that develops has
receptors that are mature enough at the correct time to respond to
the prostaglandin .
- If the ovulation is late in the cycle the
prostaglandin receptors are not mature at the time of endogenous
prostaglandin release, so luteolysis of this corpus luteum does not
occur and there is a prolonged diestrus. This may also explain why
prostaglandin administration is not always effective in mares.
Persistent corpora lutea,
also termed pseudopregnancy or spurious pregnancy.
- This is a prolonged corpus luteum life span
that may occur without uterine pathology.
- This condition can occur with or without
breeding and is the number one cause of anestrus in mares.
- The average duration is 35 -90 days.

Note the persistent diestrus as indicated by the prolonged high
progesterone.
-
Proposed mechanisms
- Late diestrus ovulation with an immature corpus
luteum at the time of prostaglandin release, as described above.
- Failure of endometrial release of prostaglandin
because of endometrial pathology.
- Early pregnancy loss can also cause this
condition. Ultrasound examination may help rule this out.
- Follicular development and even ovulation
(without estrus) may continue to occur.
-
Diagnosis
- Diagnosis is by palpation for uterine tone and
follicular activity in a non pregnant mare.
- You can ultrasound to make sure the mare is non
pregnant.
-
Treatment
- Prostaglandin should lyse the corpus luteum and
bring the mare back into heat.

Lactational anestrus
- The ' 9 day' or 'foal heat' is usually readily
observable, but subsequent heats may not be readily observed. This
is usually a result of subestrus because of the mare being so
concerned about the foal.
- However, this may also be a persistent corpus
luteum.
- May be due to seasonal anestrus if the mare
foaled very early in the year
- May be due to other unknown causes
-
Diagnosis
- Progesterone analysis and/palpation will
usually be able to determine if the mare is cycling normally.
Granulosa-theca cell tumor
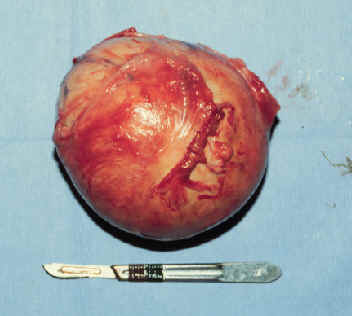

- This is the most common ovarian tumor of mares.
- It is referred to as a sex cord stromal tumor and includes granulosa
cells, theca cells with Leydig and Sertoli-like cells occasionally
noted.
- These tumors are endocrinologically active with variable
production of gonadal steroids.
- There is limited tendency for
metastasis in mares.
- There is no age distribution. They have been
reported in mares as young as 2 yr old.
- This is the only tumor that
causes estrus behavioral changes. Mares may exhibit anestrus,
continuous or intermittent estrus or stallion-like behavior.
- Diagonsis
- On
palpation per rectum, an enlarged firm ovary is found with the
opposite ovary small and inactive due to lack of gonadotropin
stimulation resulting from inhibin production by the tumor. The
affected ovary typically lacks a palpable ovulation fossa (although
with very large ovaries, this can be hard to discern).
- On ultrasound
exam, the typical appearance is multiloculated, although there is
much variation.
- Probably the most definitive diagnostic tool is the
inhibin assay (presently done at UCD). A granulosa cell profile is
done in which inhibin is assayed along with progesterone and
testosterone.
- anti-Müllerian hormone (AMH)
strongly expressed by granulosa cells in equine GCT and
in normal antral follicles. - may be a useful biomarker
for detection of GCT in the horse (Ball UCD).
- It is important to differentiate this condition from
an ovarian hematoma.
- With a hematoma, the mare continues to cycle,
an ovulation fossa is present (but may be hard to palpate if the
hematoma is very large).
- The opposite ovary is normal in size and
activity.
- The hematoma will regress with time and may respond to PGF
with a decrease in size.
- With a hematoma, inhibin and testosterone
are low.
- Treatment of a granulosa cell tumor is surgical
removal.
- Removal leads to resumption of normal activity in the
remaining ovary in most mares within 2-16 mos. post-op (ave, 6 mos).
-
The time depends on how long the tumor has been present. The
prognosis for future fertility is as good as before the tumor
developed.
Other ovarian tumors found in mares
include:
- Dysgerminoma: This is a malignant ovarian tumor
of germ cell origin. There is rapid metastasis to the abdominal and
thoracic cavities. Typical history is of chronic weight loss and
abdominal discomfort. On exam, an enlarged multilobulated ovary or
abdominal mass is found.
- Teratoma: These are benign tumors of germ cell
origin. They may (and often do) contain teeth, hair and bone. They
are usually an incidental finding at slaughter or necropsy. They are
usually small and nonpalpable and do not affect fertility.


- Serous cystadenoma: These are benign primary
epithelial ovarian tumors. They typically have a gradual onset and
the affected ovary contains palpable cystic areas on its surface.
The other ovary is unaffected.
Anovulatory Hemorrhagic Follices
- Hemorrhage into follicular lumen before
ovulation
-
May be about 8%
incidence
- Formation of luteal tissue minimal
- Regress over time
- Often observed in autumn
- Ultrasound appearance
- Thick walled
- Free floating spots in antrum as follicle
develops
- Once growth stops, contents become “organized”
– echogenic with fibrin strands
- May luteinize to some degree
- Older mares
- Treat - wait and/or prostaglandin
-
Article - click here for
more information.
Constant estrus
- Constant estrus may just be an over
interpretation by the owner of the mares actions. Urinating and
winking do not always mean estrus.
- Vaginal irritation may make a mare wink and
appear to be estrus.
Nymphomania
True
- True nymphomaniacs have normal cycles, have
abnormal CNS signs at estrus.
- They may be mild and be completely normal
except during estrus. These mares may be too crazy to breed.
- Severe nymphomaniacs have constant aggression
and are not in heat. They are not cystic and the ovaries are small
and hard. Ovariectomy results in no change in their behavior.
- This may be the result of adrenal production of
steroids. If so, 10-15 mg dexamethasone may suppress the signs.
Progesterone may also suppress the signs, but do not count on it.
Recently it was reported that these mare may be hypothyroid and
supplementation with thyroxine restored normal behavior.
Racing mares
- Many mares on the track are given anabolic
steroids, such as Equipoise.
- Equipoise is definitely detrimental to
stallions, however the effects on mares are much less.
- In a study (JAVMA; 186:583, 1985) when 46 mares
were given equipoise for 53 weeks, or 19 injections, the last of
which was in December, the first ovulation was at the same time, but
the conception at the first heat was lower, resulting in an overall
longer time to get the mares pregnant.
|
 Equine
Index
Equine
Index