Bovine
Postpartum
Problems
 335-348 335-348
Postparturient paralysis
- Postpartum paralysis occurs due to trauma and
associated inflammation to the obturator and peroneal nerves.
- Damage
to the obturator nerve causes the cow to be unable to rise and she
will be laying spraddle-legged.
- Damage to the peroneal nerve causes
knuckling.
- The prognosis for these conditions is fair to guarded and
depends greatly on the quality and intensity of treatment.
- Treatment
consists of nursing care and is aimed at preventing the "crush
syndrome" where nerve damage results from the weight of the cow
in prolonged recumbency. Hobbling helps cows with injury to the
obturator nerve to get around.
The postpartum period
- Immediate postpartum care (in chronological
order) consists of:
- 1)calf - check respiration, clean nostrils, rub
skin;
- 2) cow - check for presence of another fetus and damage to the
birth canal;
- 3) calf - disinfect the umbilical cord;
- 4) cow - give
oxytocin, check udder;
- 5) calf - feed colostrum (2 L) within 6
hours,
- check for birth defects.
- The postpartum period spans the time from
parturition to complete involution of the uterus. It can be divided
into 3 periods.
- The puerperal period is the period from parturition
until the pituitary is responsive to GnRH (usually 7-14 days
postpartum).
- The intermediate period begins with the increasing
sensitivity of the pituitary to GnRH and lasts until the first
ovulation (14-20 d pp).
- The post-ovulatory period is the time from
the first ovulation until involution is complete.
Normal involution
- For the first few days after parturition, it is
impossible to palpate the entire uterus, but you can feel a thick
uterine wall and longitudinal ruggae. A thin walled, flaccid, smooth
uterus is abnormal.
- By approximately 2 weeks postpartum you should
be able to palpate the entire uterus. A discharge (called "lochia")
is normal during this time. It should be odorless, thick, reddish
(tomato soup), and may have white flecks. The caruncles will slough
around 7 days postpartum. The fluid should be gone by 18 days and
the uterus normal size by 5 weeks. Epithelization of the caruncular
sites is complete by 40-50 days.
Abnormal
postpartum period
- One of the main causes of abnormal involution
is an unsuitable calving environment.
- The ideal environment is a
sunny, grassy well drained pasture.
- When cows are calved repeatedly
in a confined area, "Seeding" of the area with pathogens
may occur, thereby increasing the incidence of postpartum metritis.
- Inappropriate obstetrical practices, abortion diseases and retained
placenta may also contribute to the problem.
- An abnormal postpartum
uterine involution is often associated with other primary problems,
e.g. LDA, ketosis, mastitis.
- Dairy cattle tend to have a higher
incidence of postpartum problems than do beef cows.
- Many problems
can be prevent by hygiene.
Puerperal metritis
- This condition occurs within the few days just
after calving.
- Clostridia
is often involved but other pathogens such as coliforms, etc. may be
involved as well.
-
Puerperal metritis is associated with uterine
atony or inertia, with or without retained fetal membranes.
-
Cows
will be systemically ill.
-
They will exhibit depression, anorexia, GI
atony, agalactia, will be febrile, and may have peritonitis.
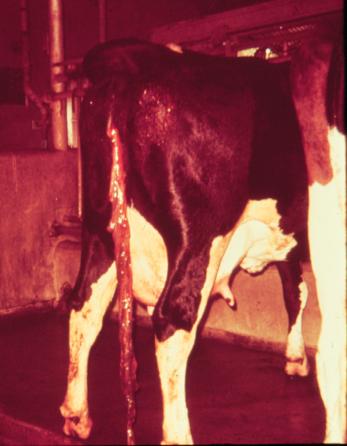
-
The
uterine discharge will be fetid, foul-smelling, watery, and
reddish-black.
-
The uterus will be thin walled and atonic.
-
This
disease can be life threatening.
-
Treatment should include both
systemic plus
intrauterine antibiotics.
-
Systemically, penicillin is a good choice,
while tetracycline is best intrauterine.
-
The uterus will be friable
so care must be taken with intrauterine treatments.
-
Uterine lavage,
consisting of draining off the fluid and flush the uterus
atraumatically, helps to reduce the amount of debris and bacteria
within the uterus.
-
Uterine ecbolics, such as oxytocin or ergonovine
maleate may help to stimulate uterine contractions and prevent
buildup of more fluid.
Postpartum metritis
- The key differentiating feature between common
postpartum metritis and puerperal metritis is that cows with common
postpartum metritis are not clinically ill.
- In most cases, the
following bacteria which have a somewhat synergistic relationship
are found in the uterus.
- Fusobacterium
necrophorum
produces a leucotoxin,
- Bacteroides
melaninogenicus
and fragillus
produce and release a substance which prevents phagocytosis.
- Actinomyces
pyogenes
produces a growth factor for Fusobacterium.
-
Other bacteria can cause a postpartum metritis but rarely persistin
the uterus, cause permanent damage or infertility.
- Incidental
bacteria are usually gone from the uterus by 3 weeks.
- A.
pyogenes
causes extensive damage if present for greater than1 week. After
clearing the uterus of A.
pyogenes
it takes at least 1 mo. to resolve the damage and restore fertility.
- The problem of delayed involution or metritis
is usually detected on rectal palpation.
- Often no systemic signs are
seen.
- A purulent discharge may be observed.
- Upon vaginal speculum
exam a discharge from the cervix, along with inflammation of the
cervix and vaginal wil lbe seen.
- In a California study they concluded
that a speculum exam was better than palpation for the diagnosis of
metritis.
Treatment
- Treatment will vary depending on the particular
situation (cow, client, etc.).
- One alternative is to do nothing,
just monitor the cow and intervene only if she shows systemic signs
or the condition persists at the end of the Voluntary Waiting
Period.
- Cows seem to do as well with non-intervention as with
aggressive treatment and the problem of withholding milk because of
residues is avoided.
- Another treatment alternative which does not
involve dumping milk is ProstaglandinF2alpha.
- Studies have shown that treatment with Prostaglandin gave equal or
greater fertility than that obtained after intrauterine therapy,
regardless of the drug used IU.
- In addition to causing luteolysis,
Prostaglandin may stimulate myometrial contractions, may stimulate
phagocytosis by uterine leucocytes and decreases progesterone
inhibition of uterine defense mechanisms.
- Other hormones which have been used include:
- Estrogens, are sometimes used because they
stimulate uterine defense mechanisms, however there is concern that
they also open the utero-tubal junction.
- Long acting forms (such as ECP) may result in
salpingitis, myometrial infection, and subsequent decrease in
fertility. It has been reported that 5 mg estradiol benzoate given
after 5 d postpartum increases uterine phagocytosis without
undesirable side effects.
- The potential benefits of GnRH are related to
the involution of the uterus and the level of management. Use of
GnRH during the postpartum period may result in an increase in
pyometras.
- Intrauterine antibiotics:
- Oxytetracycline intrauterine is effective, but
there is some concern that it may decrease uterine defense
mechanisms.
- Although it is slightly compromised by organic debris,
you can achieve MIC in the uterus with intrauterine administration,
but not with systemic administration without nephrotoxicity.
- Not shown to improve
reproductive efficiency
- None aproved
- Other antimicrobials are generally not as
effective as tetracycline.
- The aminoglycosides are not recommended.
They require an aerobic environment, but the uterus is anaerobic.
The presence of organic debris inhibits their efficacy. Importantly,
their use in food animals is prohibited.
- The sulfonamides are
ineffective in the presence of organic debris, of which there is
usually copious amounts.
- Penicillins are usually ineffective by the
intrauterine route because penicillinase producing organisms are
present early on (during the first 3 weeks).
- In the past,
nitrofurantoins (nitrofurazone) has been widely used as an
intrauterine infusion, however it is ineffective in the presence of
organic debris and you cannot achieve the MIC in the uterus.
Moreover, it is labelled as "Not for use in food producing
animals".
- Exenel (ceftiofur) -
- 2.2 mg/kg SID
5days efective
- Approved for metritis

- No withdrawl
- Cure rate for the 1.0 mg ceftiofur
equivalents/lb (2.2 mg/kg) BW dose group was significantly
improved relative to cure rate of the negative control on
day 9.
- Ceftiofur hydrochloride administered
daily for five consecutive days at a dose of 1.0 mg
ceftiofur equivalents/lb (2.2 mg/kg) BW is an effective
treatment for acute post-partum metritis.
Retained Fetal Membranes
- This is usually defined as failure of placenta
to be released by 12 hours postpartum, although some use 24 hours as
the cutoff.
- The incidence generally ranges from 5-10% in dairy
cattle to 1% in beef. In cases of induced parturition the
incidence increases to 30-100%.
- The detrimental effects come about
primarily as a result of the metritis caused by the retained
placenta.
- This is manifested by an increase in the days to first
service (4 days), an increase in days open (19-35 days), and an
increase in services/conception (0.2).
- There are multiple etiologies
which may be involved.
- Basically they relate to a disturbance in the
loosening mechanism in the placentomes or uterine inertia.
-
Separation of placenta requires a series of events beginning with
prepartum maturation of the placenta. During parturition, there is
mechanical detachment of the cotyledon by uterine pressure, followed
by anemia of the fetal villi after fetal expulsion and a reduction
of the size of the caruncles during postpartum uterine contractions.
Myometrial activity decreases by 24 hours after parturition and
almost ceases by 48 h, so if expulsion has not occured by 24 hours,
it is unlikely to occur until progressive liquefaction and expulsion
6-10 days later.
- There are some specific causes of retained
placenta, including premature delivery, infectious diseases,
metabolic/nutritional causes, hormonal causes and uterine inertia.
- Diagnosis is usually obvious. Retained placenta
may cause decreased appetite and decreased milk yield resulting from
acute metritis.
- Treatment decisions, although maybe considered
somewhat controversial, should be based on "do no harm".
-
If left alone, the placenta will usually drop approximately 5 days
postpartum.
- If treated, they often take longer to be released
because of reduced autolysis.
- Conservative treatment consists of
trimming the membranes off at the vulva and monitoring TPR,
appetite, milk production, attitude, etc.
- Antibiotics should be
given if the cow is sick (see puerperal metritis).
- Oxytocin is often
recommended, especially in the first 24 hours, although it may be
beneficial for 4-7 days. It has been shown to increase phagocytosis
by uterine neutrophils for up to 8 days but has not been shown to
hasten release of a retained placenta.
- Manual removal is not
advised.
-
Manual removal is associated with decreased fertility.
-
Numerous studies have looked at manual removal vs. other treatments
or no treatment at all and in every case manual removal had a
negative effect on future reproductive parameters.
-
The use of
chemotherapeutic agents may actually prolong the condition by
interfering with uterine defense mechanisms or inhibiting the lysis
of villi.
-
Antibiotics, hormones, including estrogens (see above),
prostaglandins and oxytocin have all been used in various dosages
and treatment schedules all without significant effect on releasing
retained placentas.
-
Basically, if the cow isn't sick, leave her
alone, if she is clinically ill, treat the illness.
- Prevention is recommended.
- Try to have dietary
calcium <100 g/d for the last few wks of the dry period.
- Vitamin
E at a level of 0.74 g/d per os during dry period
- Se at 0.1
mg/kg i.m., 21 days prepartum will lower the incidence of retained
placentas.
- A good review of this subject is: Paisley
LG, Mickelson WD, Anderson PB; Mechanisms and Therapy for Retained
Fetal Membranes and Uterine Infections in Cows: A Review.
Theriogenology 25 (March 1986):353-381
Pyometra
-
Accumulation of pus in the uterus
-
Retained CL
-
Anestrus is the primary clinical sign. There is no
vaginal discharge
-
Etiology
-
Postpartum - fluid or infection in the uterus when
ovulation and CL forms.
- Early ovulation or delayed fluid clearance
may increase the problems
- Postcoital - almost pathognomonic for
Trichomoniasis
-
Diagnosis
-
Rectal palpation
-
Fluid filled uterus, fluid flows from horn to horn
-
CL present
-
Absence of positive signs of pregnancy (diff dx)
-
Vaginal exam (cervix usually closed)
-
No systemic signs
-
Treatment
-
Estogens 50-65% effective
-
PGF2a 85-90% effective - increase efficacy if treat 2
days in a row
-
Intrauterine infusions
|
)
 Bovine
Index
Bovine
Index